Blood Clots: Risk Factors, Prevention and Treatment
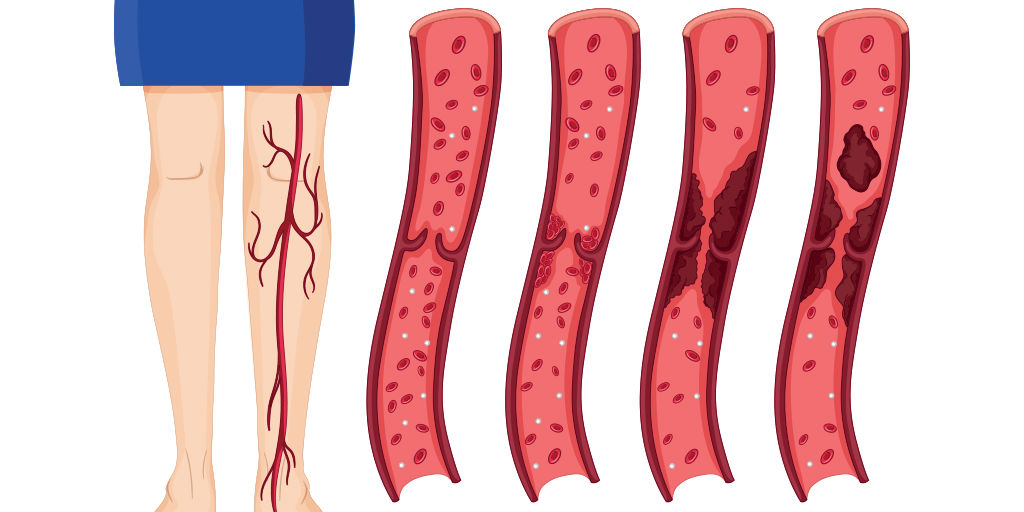
Have you ever wondered how a blood clot becomes dangerous? Generally speaking, the ability of your blood to clot is a good thing. When you get a cut, the reason you don’t keep bleeding and bleeding is that your blood contains platelets which make it thicken or “clot.” This is how your body naturally seals off a leak and begins to heal itself. Unfortunately, clots can form even when there is no cut – on the inside, in one of your veins or arteries. When this happens, the clot is called a thrombus. If some or all of that clot moves to another area of the body, it’s then called an embolus. When a clot forms in your veins or arteries, it can be very dangerous.
Compartment Syndrome
Most clots form in veins, specifically the veins in the lower legs. When a clot forms in a leg vein it may completely block the vein. If enough of the veins in a leg are blocked by the clot, the flow of blood back to the heart is reduced and the blood behind the block may begin to back up. If the veins are not re-opened, the blood begins to collect, or pool. The blood has no place to go. It simply keeps collecting and collecting until it is pushing on all the muscles as well as the veins and arteries in the leg. When this happens, the leg may begin to swell and may shut down more veins and more arteries until there is no room for new blood to get in or old blood to get out. If this process is not stopped, the leg will then turn blue and the tissue below the block can begin to die. The end result is gangrene and probably amputation of the leg. When this happens, doctors call it compartment syndrome. Losing a leg is an awful thing, but there is something even worse that clots can do.
Pulmonary Embolism
When a clot forms in a leg vein, it usually attaches to the vein wall. After a while, a clot can break into pieces or just simply detach from the vein wall. If this happens, it will circulate with the blood through the body and into the lungs where it will become lodged in one or both of the lung arteries. When this happens, it is referred to as a pulmonary embolism. A very large pulmonary embolism can cause an instantaneous cardiac arrest. A small or moderate-sized pulmonary embolus may cause no symptoms at all or may cause symptoms such as sudden shortness of breath, bluish coloration of the skin, rapid breathing, anxiety, restlessness, chest pain, spitting up blood, or a rapid heartbeat. Most of the time, if a person does not die immediately from a pulmonary embolus, he will survive unless he has a second embolus.
If an embolus is large but is not immediately fatal, the blood pressure in the lung arteries rises. The right side of the heart then has to pump harder than usual because it must overcome the higher pressure and may not to be able to pump enough blood through the lungs. As the heart works harder and harder it will get bigger (enlarged heart) until it can work no more—then it simply stops. What makes a blood clot in the leg vein so dangerous is that it often doesn’t reveal itself until it has lodged in a lung artery (becomes a pulmonary embolus). And once that happens, once the symptoms show up, death is not far behind, at least with large clots. In other words, there is very little that a doctor can do to save a patient once a large clot gets to this stage. So, what a doctor must do to prevent death from a pulmonary embolism is to prevent the clot from forming in the first place.
Looking for More Information?
Download our eBook "Understanding Medical Malpractice in Plain English"
DOWNLOAD YOUR COPYBlood Clot Risk Factors
Doctors know that certain conditions are commonly associated with the formation of clots. These conditions are called “risk factors.” When a patient has a certain number of these risk factors, doctors must take steps to prevent clots from forming. Some of the risks factors for clot formation include:
- Having a close family member who has had a pulmonary embolism
- History of a heart attack or stroke
- Blood clotting disorder
- Recent surgery with anesthesia lasting longer than ½ hour
- Pregnancy, taking birth control pills or taking estrogen replacement therapy
- Fractures to the hip or legs
- Standing or sitting still for long periods of time
- Cancer
- Obesity
- Smoking
- Age, 55 years-old and older
Preventing Blood Clots
One of the best ways to prevent medical errors is by being actively involved in the care you receive. In the medical arena, the patient is king, so act like one and take charge of your care. If you have any of the risk factors for blood clot formation (fly a lot, take birth control, not active, etc) ask your doctor if you need to be concerned about blood clots. If you (or loved one) are about to undergo or have undergone a surgery, ask these questions of your doctor:
“Are you concerned about blood clots during or after surgery?”
“Why not?”
“What about the fact that I’m (on estrogen; obese, older than 50 or other risk factors you possess?)”
Ask specifically what should be done to do to prevent blood clots from occurring. Some of the things recommended may include:
- getting you quickly walking around (they call it “early ambulation”);
- using elastic stockings (these will likely be called them “TED hose”);
- using the sleeves or boots with the plastic hoses (these are called “SCD’s” or “sequential compression devices”)
- prescribing a medication that reduces clotting risk, such as Coumadin or low dose Heparin
- using a combination of some or all of the above
Regardless of what method your doctor recommends, keep in mind the following and ask questions or make demands of your doctor accordingly:
- Early ambulation means getting out of bed early in the recuperation period (day-of or day-after the surgery) AND substantial movement, such as repeated laps around the halls. Walking from bed to chair or bathroom and back is NOT enough.
- Elastic stockings have not been shown to be very effective in clot prevention and if misused can actually be dangerous. Stockings should NEVER be used as the only method of clot prevention. Also, to be effective at all, they must be fully applied on the legs. They should never be rolled only part way up, or part way down. If that happens, the part that is “rolled” can act like a rubber band that squeezes the leg at one isolated junction. Instead of helping prevent clots, this rubber band effect can actually cause them.
- SCD’s (balloon-like leg/foot wraps with air hoses) have been shown to be very effective, but only when they are actually used. (They work by intermittently inflating to squeeze your legs to keep the blood flowing). The sleeves can be inconvenient to put on and off when a patient begins to walk around so sometimes nurses just leave them off. The rule is that whenever the patient is going to be sitting or lying still for more than a half hour, the boots must be applied (attached to air hoses making whooshing sound).
- Doctors used to think that the use of heparin or other medications which limit clotting could be dangerous (may cause excessive bleeding). Current research has shown such fears to be unfounded with respect to most types of surgery and with respect to most patients. If your doctor gives this reason, question it or ask for a second opinion.
The prevention method your doctor must use depends upon your risk factors. So, if you have any doubt whether your doctor is doing enough, ask questions. Get answers or get a second opinion. Take charge of your care.